Pelvic Floor Reconstruction
Intraoperative photos
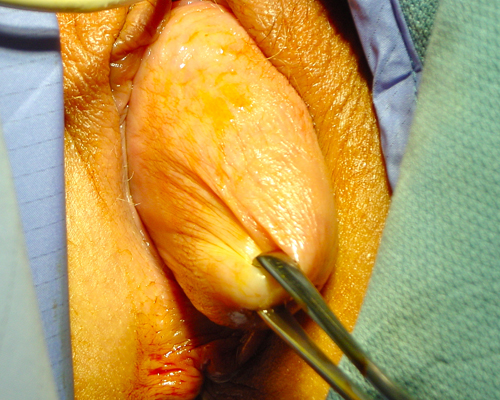
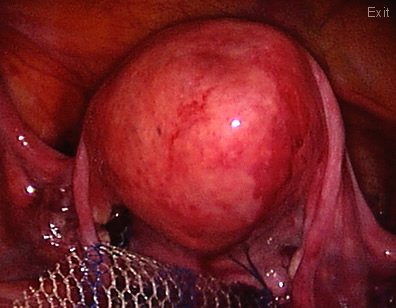
After this patient was put to sleep the prolapse is assessed and the uterus is shown to come outside the introitus.

She underwent a laparoscopic hysterectomy and complete pelvic floor reconstruction including the perineum (area between the vagina and the anus). The final result is shown.

This other patient has a very troublesome prolapse: A vaginal eversion. The vaginal canal is coming "inside out".
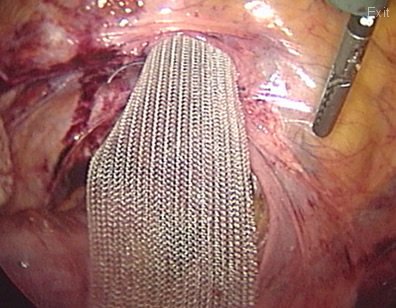
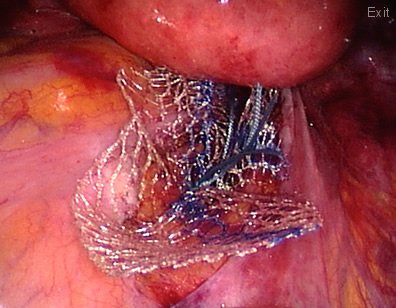
In this patient with a vaginal eversion; a mesh is attached to the vaginal vault and the vagina is pulled towards the pelvic cavity. The other end of the mesh will be attached to the sacrum bone (sacrum promontorium) to restore the normal anatomy.
The mesh is being deeply buried "between the cavity and the bones". This will avoid contact of the mesh to the bowels.

Finally any low vaginal wall defect is repaired vaginally and a pack (to prevent bleeding) is inserted into the new vagina for 24 hours. A small tube (catheter) is also seen coming from the urethra to allow a free passage of urine. A very good result is shown on this picture. This patient was discharged home 2 days after her surgery.
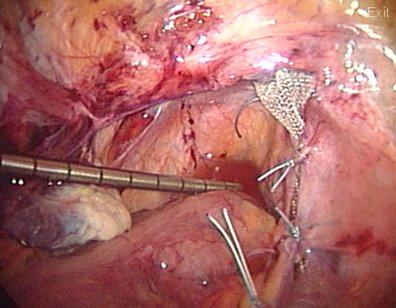
In a different patient with a uterine prolapse, who wants to preserve fertility, a mesh is used to reconstruct the pelvic floor.
The mesh is also attached to the uterosacral ligaments (that normally suspend the uterus to its normal position)
The mesh is attached to the sacrum (tail bone) and buried between the lining of the pelvis and the bones. The uterus is seen back to its normal position in the pelvis.

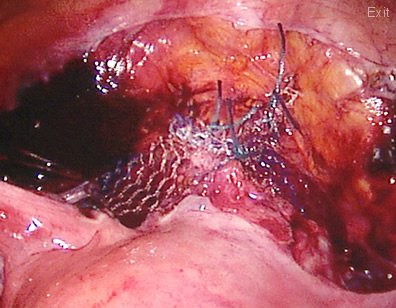
The whole of the vagina has been reconstructed including the perineum (area between the introitus and the anus) to provide full support. A "transversal" tape or sling has also been placed under no tension underneath the urethra (opening from the bladder to pass urine) to correct incontinence.